
POSTERIOR IMPINGEMENT IN DANCERS
Posterior ankle impingement is a common cause of pain in ballet dancers. Other names for this condition are “os trigonum syndrome” and “nutcracker syndrome”. It is called “nutcracker syndrome” not because of its common occurrence in ballet at Christmas-time but because of the way the tissue of the ankle is squeezed at the ankle. The following is a brief overview of this condition and how it relates to dancers.
Posterior impingement of the ankle is often attributable to the presence of an accessory bone growth called an os trigonum or a Stieda process that is located just behind the talus (see x-ray for anatomy). The stress from repetitive plantarflexion by dancers, especially at a young age, is the suspected cause of the development of the os trigonum. Pain in posterior impingement occurs when the soft tissue of the ankle is pinched between the posterior lip of the tibia and the calcaneus. This occurs when the foot is in extreme plantarflexion such as during releve in the demipointe or en pointe positions.
Diagnosis


Proper diagnosis of posterior impingement is imperative for recovery from this injury. Posterior impingement attributable to an os trigonum is usually misdiagnosed as Achilles’ tendonitis/tendonopathy, peroneal tendonitis or flexor hallucis longus strain.
The two main symptoms of posterior impingement are a decrease in plantarflexion compared with the unaffected ankle and pain in the posterior region of the ankle. Often dancers are aware of a lack of ability to fully pointe in one foot compared to the other, this may be an early sign of impingement. Another common description dancer’s use is it feels like pinching in the heel during releve. Diagnosis is often aided by x-Rays of the ankle. It is best to request an x-ray to be taken during releve to evaluate the biomechanics of the injury. If there has been persistent pain for a period of 1– 4 months, local swelling, and radiographic assessment indicating a posterior ankle impingement, then an MRI should be performed.
Treatment for Posterior Impingement of the Ankle
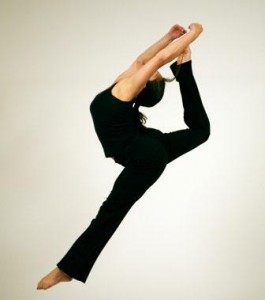
Once posterior impingement is diagnosed focused treatment should begin. Non-surgical care is usually successful and should be the first line treatment. Treatment should be focused on taking pressure off of the tissue being pinched. Exercises should focus on engaging the deep muscles of the leg especially the deep flexors. One exercise that is helpful and can be done at home is a self traction maneuver with plantarflexion (see picture). The patient holds his or her ankle, as shown, with downward pressure and performs the motion with a bent knee. Bending the knee helps disengage the gastrocnemius muscle and soleus forcing the deep flexors to engage.  Another great exercise is ankle range of motion with traction applied by a therapist using very strong elastic bands. Dancers may experience relief with traction and feel they are able to fully plantarflex; this can also be a good way to support the diagnosis as Achilles’ tendonitis is often unchanged with traction. Manipulation of the ankle especially the talus can provide relief as well. Conservative therapy is successful in the majority of cases. Recovery may take several months.
Another great exercise is ankle range of motion with traction applied by a therapist using very strong elastic bands. Dancers may experience relief with traction and feel they are able to fully plantarflex; this can also be a good way to support the diagnosis as Achilles’ tendonitis is often unchanged with traction. Manipulation of the ankle especially the talus can provide relief as well. Conservative therapy is successful in the majority of cases. Recovery may take several months.
A surgical approach should only be adopted in the following cases:
- recurrent or unremitting symptoms in professional ballet dancers;
- persistent decreased plantarflexion compared with the unaffected ankle;
- failure of physical and medical therapies after 1– 4 months (depending on the level of the athlete/dancer);
- posterior impingement clinically suspected and indicated by both x-ray and MRI.
Ankle pain and heel pain is a common symptom in dancers and posterior impingement is only one of the causes. If you think you may be suffering from posterior impingement seek advice from a qualified healthcare professional with expertise in dance injury.
-Dr. Rose, DC, CCSP®
Dr. Rose is a Certified Chiropractic Sports Practitioner® with experience in dance medicine. He is currently Director of Physical Rehabilitation at Ballet San Jose and a member of the International Association of Dance Medicine and Science.
REFERENCES
Albisetti W, Ometti M, Pascale V, De Bartolomeo O: Clinical evaluation and treatment of posterior impingement in dancers. Am J Phys Med Rehabil 2009;88:349–354.
Niek van Dijk C: Anterior and posterior ankle impingement. Foot Ankle Clin 2006;11:663– 83
F Cilli, M Akcaoglu: The incidence of accessory bones of the foot and their clinical significance. Acta Orthop Traumatol Turc 2005;39:243– 6

")




